Proper Analytical Science
With thanks to Dr Herman Edeling for compiling this content.
COVID-19 “VACCINES” – EFFICACY and SAFETY SUMMARY of FACTUAL and SCIENTIFIC MEDICAL EVIDENCE
Over the past weeks and months, one has been inundated with requests by employees, students, parents and lawyers for medical advice and evidence relevant to the risks and benefits of Covid-19 “vaccines”.
This analytic report, compiled in March 2022 and provided as a service to the public, may be shared freely and may be used in its entirety by anybody in any forum. It has been compiled as a summary of essential factual and scientific evidence, in the expectation that it will be readily understandable by all.
It is envisaged that this report will provide a useful factual basis for informed decision-making by potential recipients of “vaccines” when considering whether to give or withhold informed consent, as well as by those who feel the need to encourage or coerce others to be “vaccinated”.
If this report is to be served in legal proceedings, one would be willing to attest under oath to the contents thereof, and to supplement this brief summary with further evidence.
Part A: MEDICAL EVIDENCE RE EFFECTIVENESS OF COVID-19 “VACCINES”
QUESTION 1. ARE THE COVID-19 “VACCINES” EFFECTIVE AT PREVENTING INFECTION BY AND TRANSMISSION OF THE SARS-COV‑2 VIRUS (PROTECTION OF SELF AND OTHERS)?
Scientific Evidence Supporting Effectiveness at Prevention of Infection and Transmission
When the Pfizer mRNA “vaccines” were awarded EUA (emergency use authorisation) by the United States FDA (Food and Drug Administration), it was widely publicised that the new mRNA technology was 95% effective at prevention of transmission of the SARS-CoV‑2 virus. This claim was made on the basis of a single Pfizer trial, dated 31 December 2020, which has not been independently verified. The subsequent 6‑month data report of Pfizer, dated 15 September 2021, found a gradual decline in vaccine efficacy, at that stage claimed to be 91.3%.
Independent analyses of these Pfizer trials have since found significant flaws in the trial methodology. These flaws included failure to follow established protocols, periods of observation that were too short to reliably evaluate efficacy or safety, inappropriate demographics of the study population, premature unblinding and crossover, failure to track biomarkers, wrong clinical endpoints, failure to actively track and record the health status and adverse events of all trial participants, and use of the so-called RRR (relative risk reduction) criterion instead of the more appropriate criterion of ARR (absolute risk reduction). Application of the ARR criterion to the Pfizer 2 months data found that the absolute risk reduction was only 0.84%.
Despite these flaws, one has been bombarded by a steady stream of assurances by “authoritative experts” and their followers, proclaiming as a mantra, that “the vaccines are safe and effective”. What one has been expecting, but not heard or seen from these “experts” or their followers, is actual evidence of efficacy of the mRNA “vaccines”.
Responses to repeated questions, seeking factual or scientific evidence from “experts” who proclaim the “safe and effective” mantra, have been limited to one or both of:
- Emphatic and often angry repetition of the opinions of themselves and/or others that “the vaccines are safe and effective”, without provision of any evidence or reasons to support these opinions.
- Published studies that seem, at face value, to support an element of the mantra, but which, on closer inspection, are found to be weak and/or flawed. Such cherry-picked studies upon which supporters of the “safe and effective” mantra have relied, as have come to one’s attention, have been found to share common flaws or weaknesses, such as inappropriately selected: demographics of the study population, clinical endpoints, time of onset, and/or short timeframes of observation.
- Potentially misleading consequences of inappropriately selected demographics of the study population arise when the study population is young and/or healthy, and the data derived from such study is used to motivate administration of the “vaccine” to people who are old and/or sick. Other potentially misleading consequences of the above flaw arise when the study population has excluded pregnant females, and the data derived from such study is used to motivate administration of the “vaccine” to pregnant females.
- Potentially misleading consequences of inappropriately selected clinical endpoints arise when selected clinical endpoints are limited to “a positive test for SARS-CoV‑2”, and/or “hospital admissions for Covid-19”, and/or “death from Covid-19”; instead of proper scientific endpoints such as “all cause morbidity” and/or “all-cause mortality”. In this regard one refers inter alia to a July 2021 research article published in “Trends in Internal Medicine. Citation: Classen B. US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, “All Cause Severe Morbidity”. Trends Int Med. 2021; 1(1): 1 – 6.
- To illustrate the potentially misleading consequences of inappropriately selected time of onset and timeframes of observation, one refers to real world South African data from https://ourworldindata.org/covid-cases. According to this source the Covid-19 1st wave in South Africa peaked on 19 July 2020, with 209 cases per million people; followed by a natural decline, with only 27 cases per million people 2 months later on 19 September 2020. On 11 November 2020 South Africa recorded 28 cases per million people, and 2 months later, on 11 January 2021, the Covid-19 2nd wave in South Africa peaked with 317 cases per million people. Against this background, and by way of obviously ridiculous example:
- Had one commenced a 2‑month study in South Africa on 19 July 2020, for example to test the effect of painting the fingernails of South Africans blue with the intention of preventing transmission of the SARS-CoV‑2 virus, the above data may have been interpreted to indicate that painting fingernails blue protects against transmission of the SARS-CoV‑2 virus.
- Had one commenced a 2‑month study in South Africa on 11 November 2020, for example to test the effect of painting the fingernails of South Africans red with the intention of preventing transmission of the SARS-CoV‑2 virus, the above data may have been interpreted to indicate that painting fingernails red exhibits a negative effectiveness, by actually increasing the risk of transmission of the SARS-CoV‑2 virus.
Conclusion: One has found no reliable scientific evidence to support the notion that the Covid-19 “vaccines” are effective at preventing infection by or transmission of the SARS COV 2 virus.
Scientific Evidence Finding Against Effectiveness at Prevention of Infection and Transmission
One has read, and previously made publicly available, copies of numerous scientific articles that have found that the Covid-19 “vaccines” are not effective at prevention of infection or transmission of the SARS-CoV‑2 virus. Examples of such scientific articles can be found at https://emlct.com/index.php/covid-19-documents/, where each document bearing the prefix “NE” provides scientific evidence that the Covid-19 “vaccines” are not effective.
Conclusion: An abundance of scientific evidence finds that the Covid-19 “vaccines” are not effective at preventing infection by or transmission of the SARS-CoV‑2 virus.
Real World Factual Data re Effectiveness at Prevention of Infection and Transmission
As noted above there is scientific evidence, in the form of expert opinions and study findings, that claims to find both for and against the effectiveness of Covid-19 “vaccines”. Looking beyond the scientific evidence, at least some of which is flawed, one turns to real-world factual evidence, which cannot be said to have been planned, calculated, bought, or distorted to prove a particular point.
According to https://ourworldindata.org/covid-vaccinations, which has obtained its South African data from the South African Ministry of Health at https://sacoronavirus.co.za/latest-vaccine-statistics/, mass administration of vaccines in South Africa commenced on about 1 May 2021. According to the same source 29% of South Africans had been fully “vaccinated” by 18 March 2022, with an additional 6% partly “vaccinated”, i.e. a total of 35% of South Africans having received one or more doses of the Covid-19 “vaccines”. Of these, about 75% had been the Pfizer/BioNTech product about 25% the Johnson & Johnson product.
To illustrate the effectiveness or otherwise of the Covid-19 “vaccines” in South Africa, one refers to real world South African data from the same source, at which the following graph can be viewed and interrogated online at https://ourworldindata.org/covid-cases. The data shows that the 1st wave of Covid-19 cases in South Africa peaked on 19 July 2020, with 209.58 cases per million people; and the 2nd wave peaked on 11 January 2021, with 317.14 cases per million people. Both of these waves occurred prior to the onset of mass “vaccination” in South Africa. The data shows that, subsequent to the commencement of mass vaccination, the 3rd wave in South Africa peaked on 7 July 2021, with 329.21 cases per million people; and that the 4th wave peaked on 17 December 2021, with 390.35 cases per million people.QUESTION 1. ARE THE COVID-19 “VACCINES” EFFECTIVE AT PREVENTING INFECTION BY AND TRANSMISSION OF THE SARS-COV‑2 VIRUS (PROTECTION OF SELF AND OTHERS)?
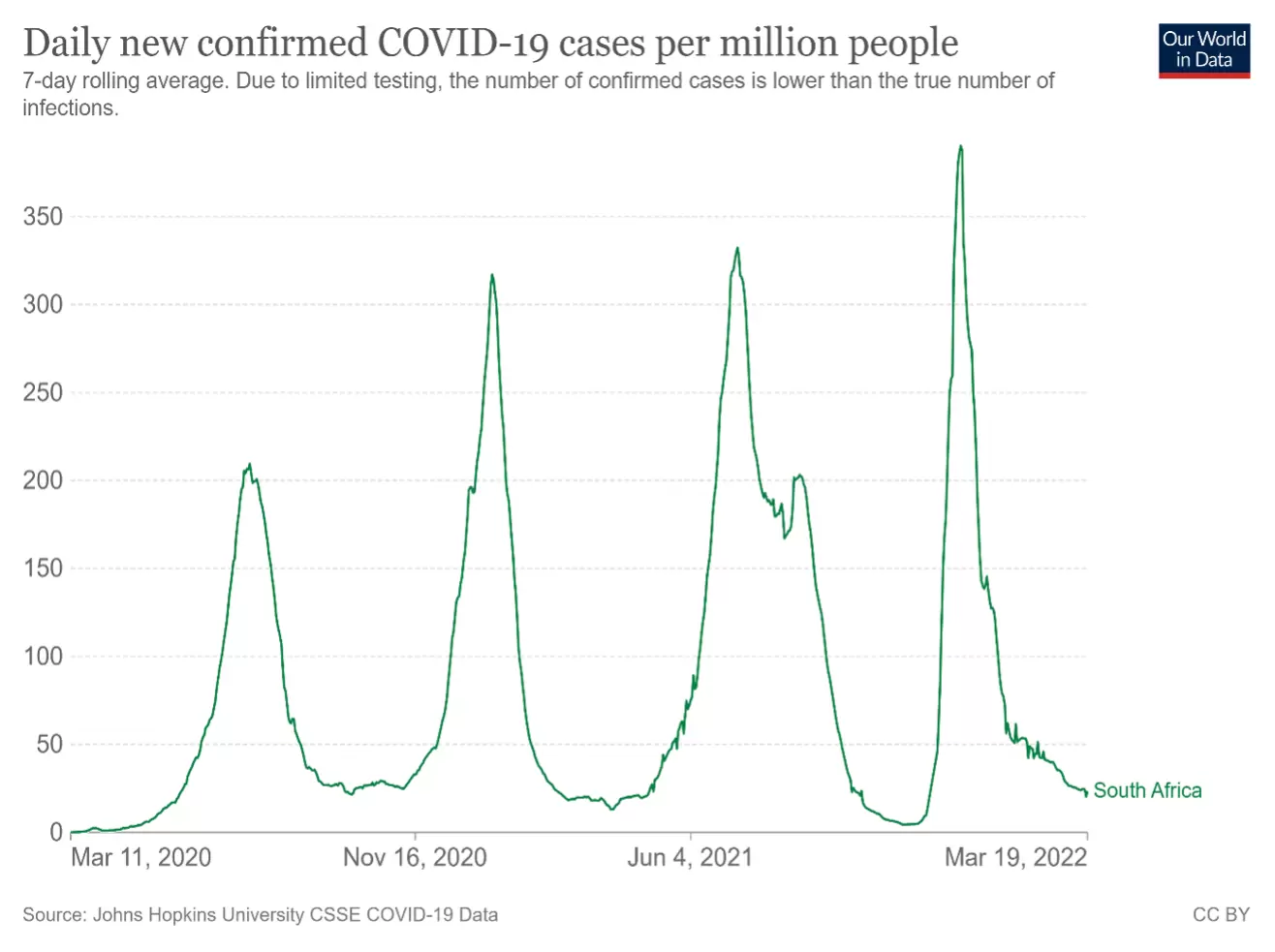
Conclusion: This data does not demonstrate any discernible benefit of the “vaccinations” to date in South Africa. If anything, the data indicates a negative benefit.
The above analysis is, of course, hampered by the low percentage of “vaccinated” individuals in South Africa. For this reason, one turns to data from other countries that are more highly vaccinated.
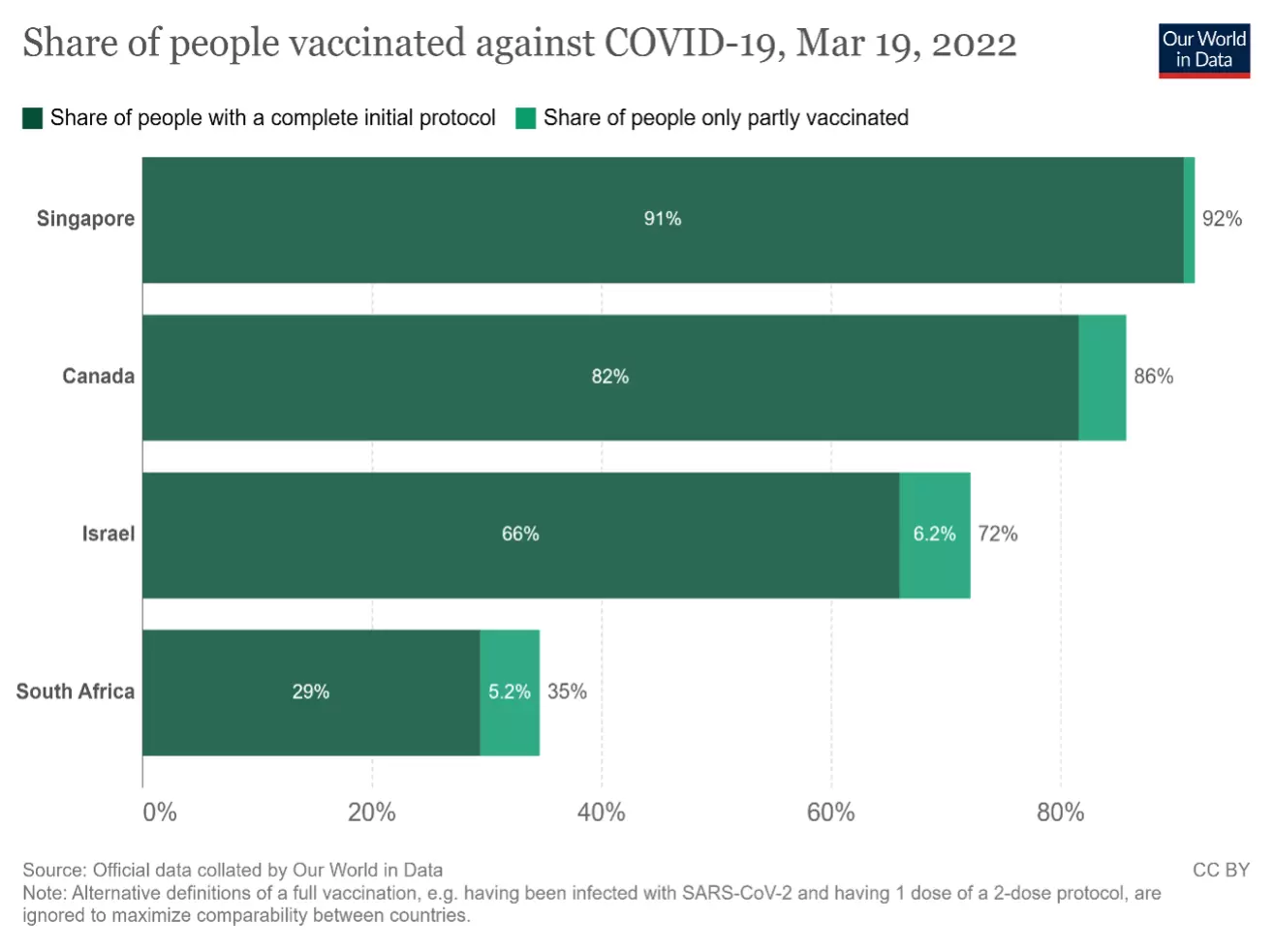
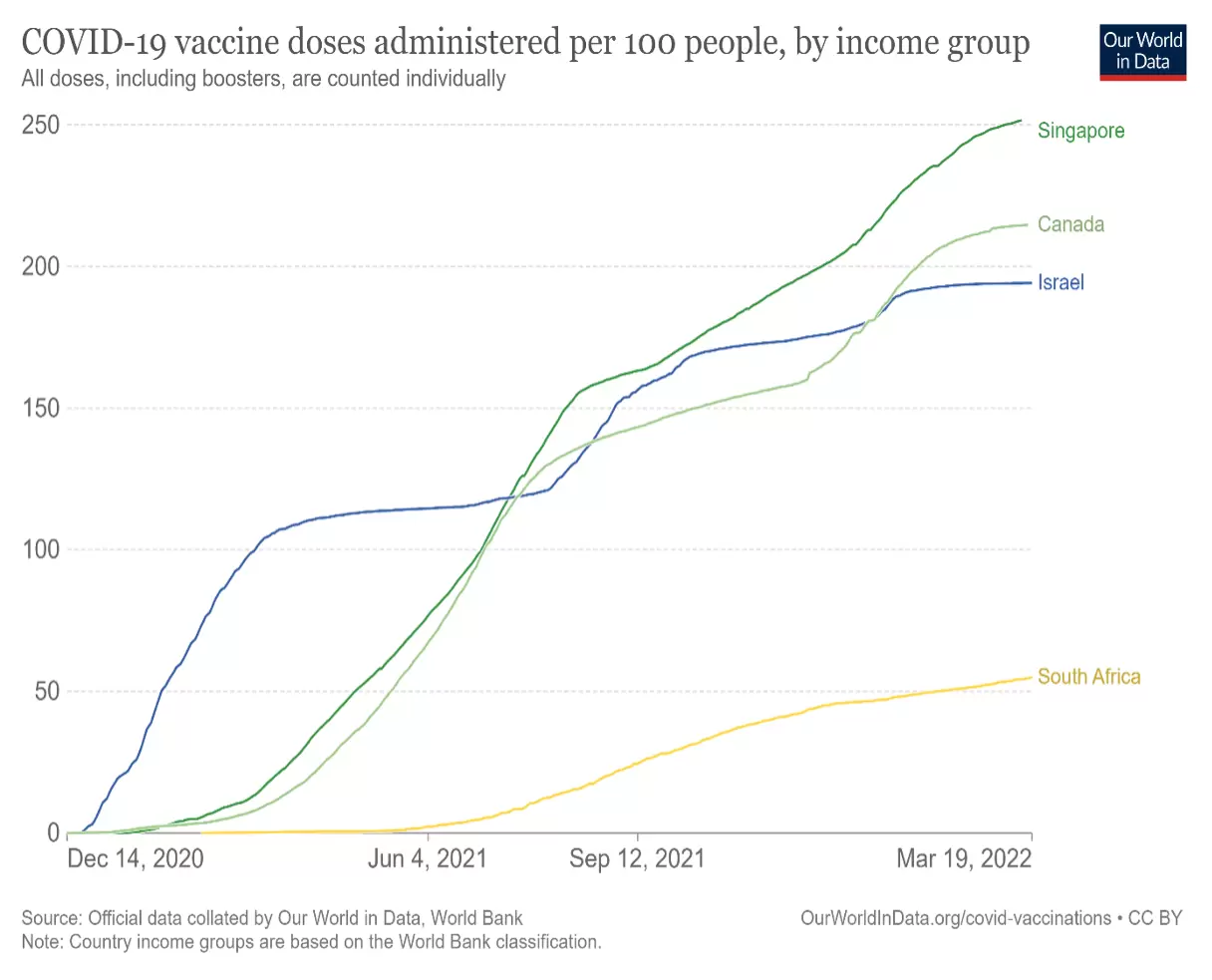
According to https://ourworldindata.org/covid-vaccinations (see chart below), by 19 March 2022. when the share of people in South Africa “vaccinated” against Covid 19 was 29%-35%, it was 66%-72% in Israel, 82%-86% in Canada, and 91%-92% in Singapore.
Then, according to the same source, mass administration of vaccines in Israel and Canada commenced during December 2020, and in Singapore during January 2021.
To test the hypothesis that Covid-19 “vaccines” are effective at preventing infection by and transmission of the SARS-CoV‑2 virus, one would expect real-world factual data in highly vaccinated countries such as Singapore, Canada and Israel to demonstrate a diminishing trend of cases over time, i.e. since January 2021. In fact, according to https://ourworldindata.org/covid-cases?country=CAN~SGP~ISR~ZAF, at which the following graph can be viewed and interrogated online, the trend since January 2021 in each of the countries shows the opposite.
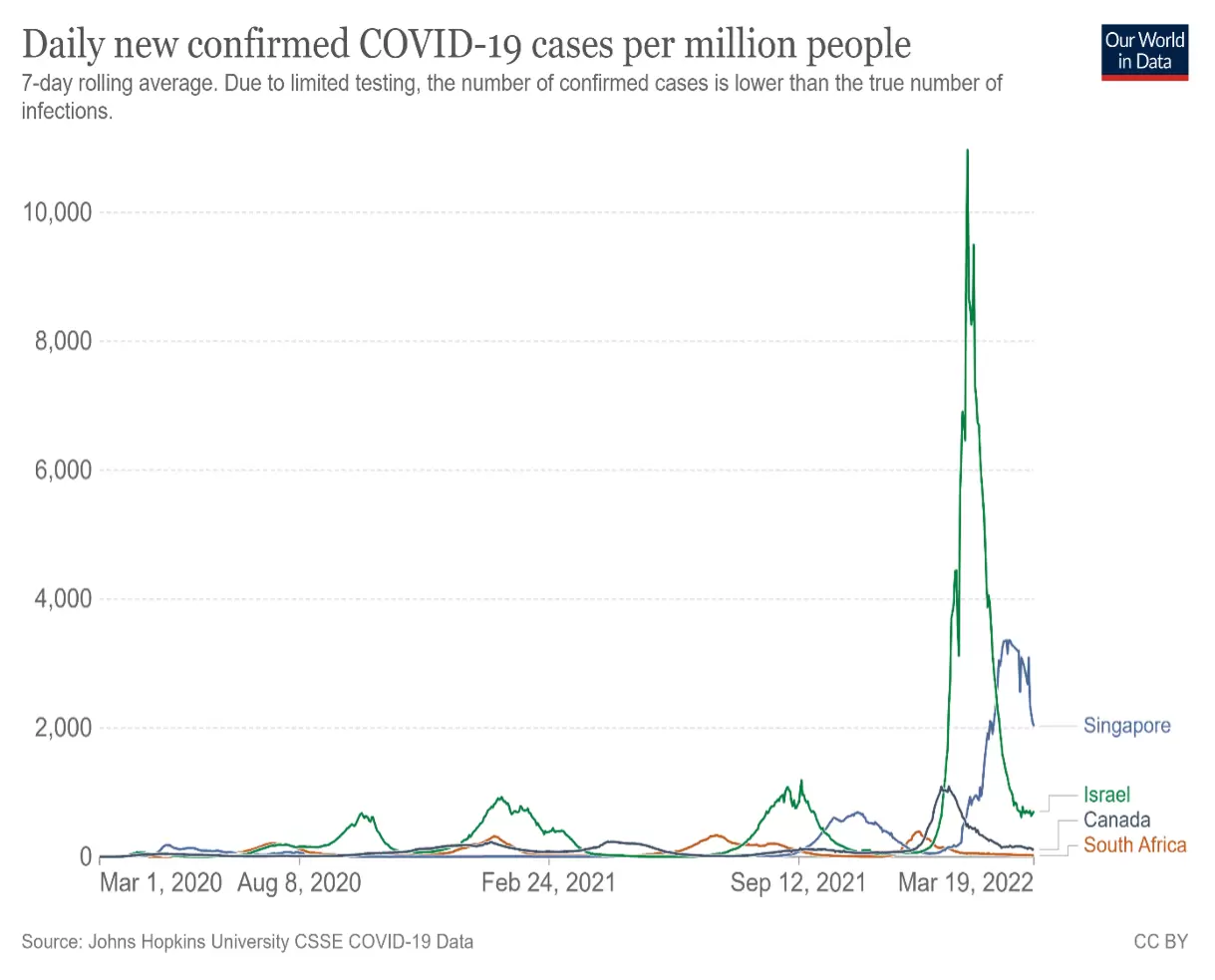
Conclusion: Again, as in the case of South Africa, the data does not demonstrate any discernible benefit of the “vaccinations” to date in any of these countries. If anything, the date indicates a negative benefit.
The above analyses relate to comparison between case numbers prior to the onset of “vaccinations”, with case numbers following the onset of “vaccinations”, in individual countries.
A further relevant comparison is evident from the above graphic, in which differences are evident between countries with higher and lower percentages of the population having been “vaccinated”. It is evident that over the past 2 months case numbers in the three highly vaccinated countries have exceeded case numbers in the less vaccinated South Africa.
Conclusion: This inter-country comparison also fails to demonstrate any discernible benefit of the “vaccinations”, and in fact does indicate a negative benefit.
QUESTION 2. ARE THE COVID-19 “VACCINES” EFFECTIVE AT PREVENTING SEVERE ILLNESS OR DEATH FROM COVID-19 (PROTECTION OF SELF)?
Scientific Evidence Supporting Effectiveness at Prevention of Severe Illness or Death
It has been interesting to observe that, as the realities set out above have begun to sink in, the “authoritative experts” and their followers have softened their stance on the effectiveness of “vaccines” in preventing infection or transmission. Instead, they have drawn another line in the sand, proclaiming as a mantra that “the vaccines are very effective at preventing severe illness and death”, even if not so effective at preventing infection or transmission.
Responses to questions, seeking factual or scientific evidence to prove the effectiveness of “vaccines” in preventing severe illness and death, have manifested the same shortcomings as described above. One therefore repeats mutatis mutandis the comments set out in paragraphs relating to “responses to repeated questions” in the previous section.
Conclusion: One has found no reliable scientific evidence, that has been collected over a suitable period of time and that has included suitable clinical endpoints, to support the notion that the Covid-19 “vaccines” are effective at preventing severe illness or death from Covid-19.
Scientific Evidence Finding Against Effectiveness at Prevention of Severe Illness and Death
In this regard one repeats, mutatis mutandis, the comments in the paragraph of the section entitled “Scientific Evidence Finding Against Effectiveness at Prevention of Infection and Transmission” above, and again refers to https://emlct.com/index.php/covid-19-documents/, where each document bearing the prefix “NE” provides scientific evidence that the Covid-19 “vaccines” are not effective.
Conclusion: An abundance of scientific evidence finds that the Covid-19 “vaccines” are not effective at preventing infection by or transmission of the SARS-CoV‑2 virus.
Real World Factual Data re Effectiveness at Prevention of Severe Illness and Death
Again, considering that scientific evidence finds both for and against the effectiveness of Covid-19 “vaccines”, and that at least some of the scientific evidence is flawed, one looks beyond opinions and studies to real-world factual evidence, which cannot be said to have been planned, calculated, bought or distorted to prove a particular point.
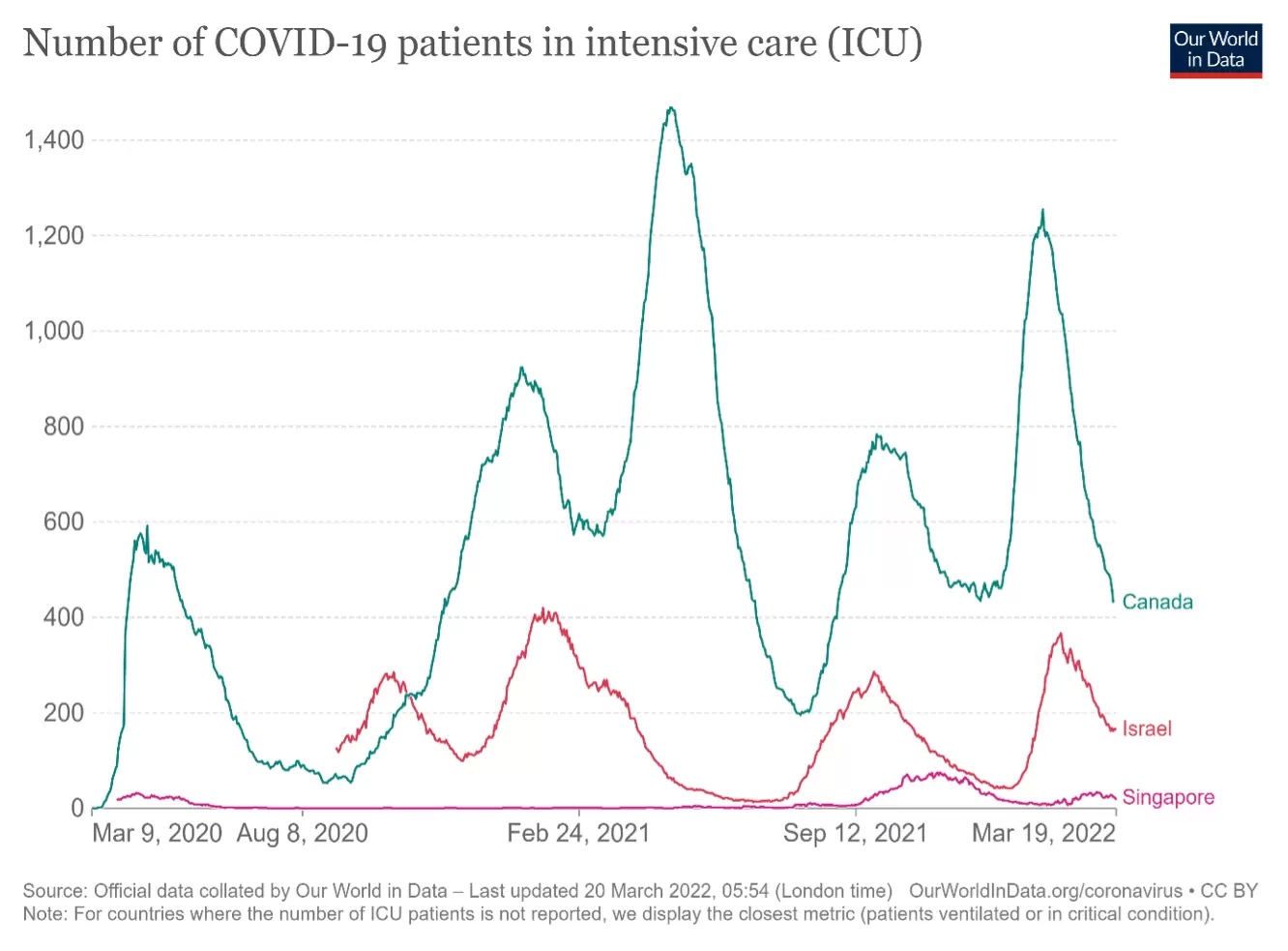
To test the hypothesis that Covid-19 “vaccines” are effective at preventing severe illness in those who contract Covid-19, one would expect real-world factual data in highly vaccinated countries such as Singapore, Canada and Israel to demonstrate a diminishing trend of cases over time, i.e. since January 2021. In fact, according to https://ourworldindata.org/covid-hospitalizations, at which the following graph can be viewed and interrogated online, the trend since January 2021 in each of these countries fails to show any negative trend. Unfortunately data for patients in ICU in South Africa is not available from this source.
To test the hypothesis that Covid-19 “vaccines” are effective at preventing death in those who contract Covid-19, one would expect real-world factual data in highly vaccinated countries such as Singapore, Canada and Israel to demonstrate a diminishing trend of deaths over time, i.e. since January 2021. In fact, according to https://ourworldindata.org/covid-deaths?country=CAN~SGP~ISR~ZAF, at which the following graph can be viewed and interrogated online, the trend since January 2021 in each of these countries fails to show any sustained negative trend.
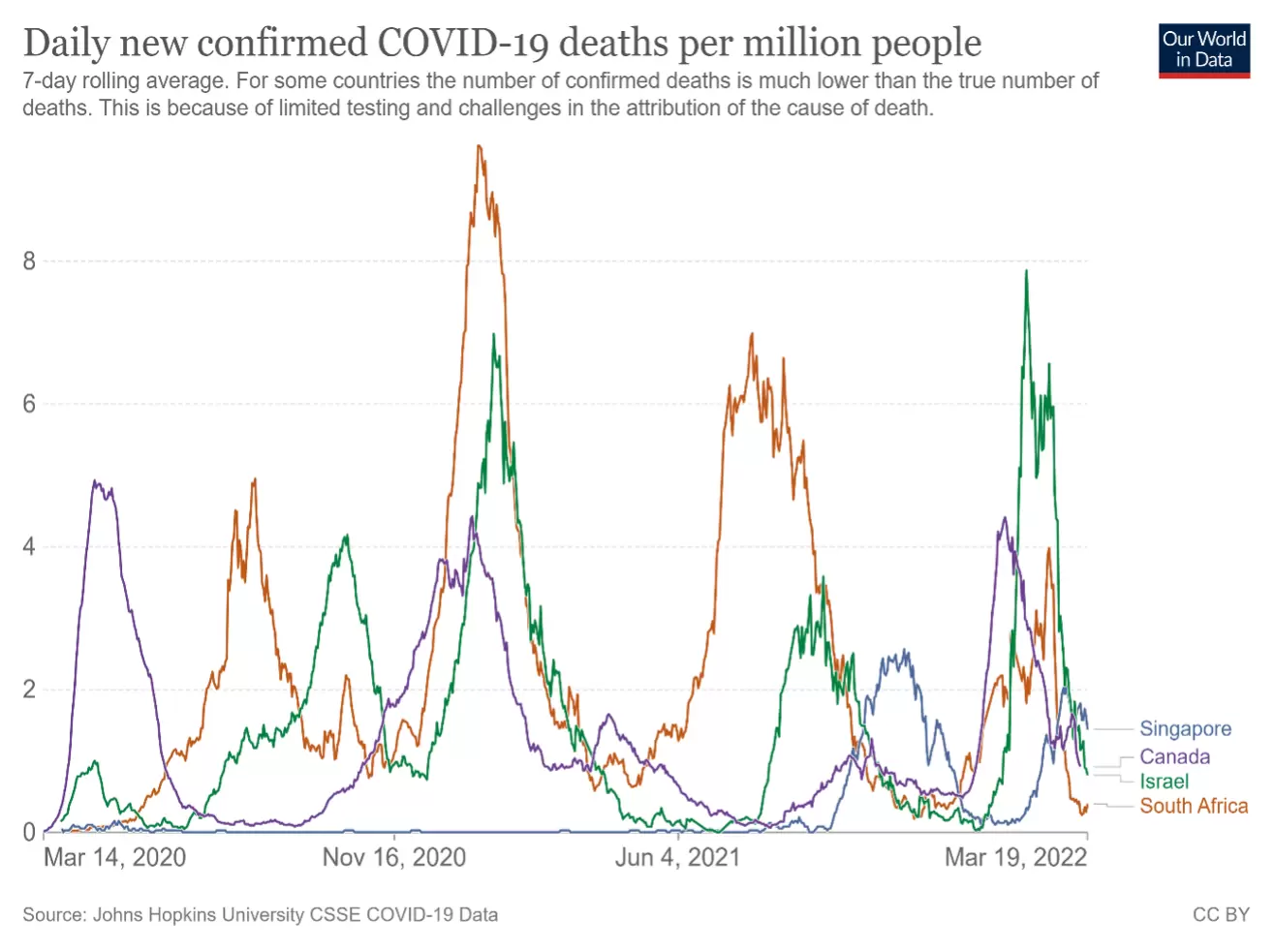
- The data from Singapore shows no benefit for the first 8 months, followed by an escalating trend of increasing deaths.
- The data from Canada and Israel show a transient diminishing trend for the first 11 months or so, followed by an escalating trend of increasing deaths.
- In contrast, the data from South Africa, which has the lowest proportion of vaccinated individuals, does show a diminishing trend of deaths over time.
Conclusion:
Real-world factual data finds no evidence to support the notion that the Covid-19 “vaccines” are effective at preventing severe illness or death from Covid-19.